
Scoliosis and Spine Program
As the only nationally ranked orthopedics program for kids and teens in Georgia*, our pediatric spine surgeons, orthotists, prosthetists and physical therapists work together to treat spine conditions in kids who are still growing.
Make an Appointment
Children’s Healthcare of Atlanta is a leader in pediatric spine care. More kids, teens and young adults come to us for spine surgery than any other pediatric hospital in the country*. Not only do we rank among the best pediatric hospitals in the country for orthopedics, but we are also the only nationally ranked pediatric orthopedics program in Georgia**.
When it comes to your child’s spine surgery, experience and outcomes matter.
Children’s performs more spinal fusion surgeries than any other hospital dedicated to treating kids and teens, with some of the best spine surgery results in the nation. We are passionately dedicated to making sure your child has the best possible outcomes.
LEARN MOREThe spine withstands a lot of stress each day, making it a common site for an overuse injury, especially in growing children. Our team of pediatric spine specialists at Children’s Healthcare of Atlanta understands how the spine can change as your child or teen grows or if your child or teen is injured.
Spine problems in children can present at birth (known as congenital spine problems), develop over time as your child or teen grows, or be caused by an injury, such as a muscle strain from physical activity or improper weight lifting. Curvature of the spine (scoliosis) can occur in otherwise healthy children for no apparent reason, although the tendency can run in the family.
If an issue arises or back pain continues in your child or teen, we recommend treatment by someone who is specially trained in caring for the pediatric spine. At Children’s, our specialists help care for, diagnose and treat spine problems in children of all ages, from birth to 18.
Scoliosis is a lateral, or sideways, curvature of the spine greater than 10 degrees. This also includes types of neuromuscular scoliosis like spina bifida, cerebral palsy, spinal muscular atrophy (SMA) and muscular dystrophy.
Kyphosis refers to the rounding of the upper back in a C-shaped curve, or a hunched back. Kyphosis most commonly affects the thoracic spine (upper and middle back) but can also involve the cervical (neck) and lumbar (lower back) portions. The two most common types of kyphosis are Scheuermann’s kyphosis and postural kyphosis. Kyphosis may also develop because of:
- Metabolic problems
- Neuromuscular conditions
- Spina bifida
- Osteoporotic fractures
- Traumatic injuries
- Slippage of vertebral disc
The symptoms of kyphosis may vary based on how severe they are. They may range from a minor change in the shape or appearance of the back to more severe nerve problems and long-lasting back pain. There may be weakness in the legs because of the pressure that is put on the spinal cord and nerve from the spinal curvature. Evaluations and diagnostic tests may include:
- A complete medical history.
- A physical examination by a doctor to evaluate spine movement, muscle strength and sensation, to help the doctor make a proper diagnosis and also rule out other similar conditions.
- Some diagnostic tests, such as X-rays, a magnetic resonance imaging (MRI) scan and a computed tomography (CT) scan, to see the structure of the spine and measure the curve.
Kyphosis has several treatment choices that range from medicines to exercises including physical therapy as well as casts and support braces. Spine surgery may also be considered in some cases.
In cases where osteoporosis causes kyphosis, it’s recommended that your child do the following to slow down the condition’s progress:
- Take vitamin D and calcium supplements.
- Use hormone replacement therapy.
- Exercise regularly.
Spondylolysis, also known as stress fractures, is a defect in the spine at a part of the bone known as the pars interarticularis. This pars region connects the front part of the backbone (vertebral body), which houses the spinal cord and nerves, to the back part of the backbone (posterior elements).
Spondylolysis is caused by genetics, overuse or repeated injuries, or a combination of the three. Children at highest risk to develop these defects are those who join in sports that require children to repeatedly arch their backs. Those sports include gymnastics, cheerleading, weight lifting and football.
Many children are symptom-free, and the condition is often overlooked. However, when spondylolysis has symptoms, it is typically lower back pain, which is made worse because of arching the back. In rare cases, your child could feel pain that goes down the legs. The pain is typically severe enough that your child may not want to join in a sport.
Spondylolisthesis, or a slipped vertebra, is commonly associated with spondylolysis. Spondylolisthesis typically occurs when someone has spondylolysis, and then as a result, one bone slips forward in relation to another.
These two conditions are the most common causes of chronic back pain in children.
At your appointment, your child’s doctor will look for signs of stress fractures by:
- Taking a complete medical history.
- Doing a physical examination.
- Getting an X-ray of the lower back.
Sometimes a computed tomography (CT) scan or a magnetic resonance imaging (MRI) scan might be used to look for very small fractures, to rule out other possible causes of pain and to plan treatment options.
A moderate approach will often work to treat spondylolysis, including rest, medication and physical therapy.
Treatment is intended to reduce pain and swelling, which usually allows the fracture to heal. In some cases, a back brace may be worn for a short time to take the pressure off the lower back. If your child’s pain continues, they may need surgery.
Trauma injuries to the spine may include spinal fractures and post-traumatic spine problems.
Acute spine injuries happen suddenly. This can be cause from things such as a car accident or a fall.
Burst fractures—thoracic or lumbar spine fractures—generally result from a high-energy impact, such as a car crash, fall from a height or contact sports. The energy of the injury causes the vertebrae to fracture, or burst, into multiple pieces, and the injured vertebrae lose height, which can lead to instability and a deformity and/or injury to the spinal cord.
X-rays of the spine, including upright or standing, are necessary to determine if the spine is stable. A CT or computerized axial tomography (CAT) scan and/or an MRI may be required for a better view of the injury.
Generally, stable burst fractures are treated with braces and pain medication. However, unstable fractures require surgery to protect the spinal cord from injury and the spine from future deformity. Any fracture-associated spinal cord compression will need surgery to decompress the cord.
Tumors and infections—such as aneurysmal bone cysts, osteoblastoma (sarcoma), histiocytosis, malignant tumors and osteomyelitis—are very uncommon.
A unicameral bone cyst, also known as a simple bone cyst, is a benign (not cancerous) bone tumor. These tumors are most commonly found near the shoulder and hip joints. They often go away without treatment after your child has completed the growth cycle.
Bone and joint infections (osteomyelitis and septic arthritis) occur much more commonly in children than in adults, with the majority of cases occurring in children under the age of 5. Our team understands these infections.
Vertebrae problems, or problems with the discs of the spine, can include degenerative disc disease, herniated discs or other disc disorders.
In recent years, disc herniation in children has become more common. A herniated disc develops when one of the discs between the bones (vertebrae) of the spine moves out of position and presses on adjacent nerves, causing pain in the back, pain in one or both legs and numbness, tingling or weakness in one or both legs. These discs are cushions that have a soft center and a hard outside. If the hard part of the disc cracks and the soft part is exposed, it is called a hernia. A herniated disc can also be called a “pinched nerve” or “bulging disc.”
Fortunately, mild to moderate vertebrae problems in kids and teens often do not require surgery. Typically conservative treatments such as rest, physical therapy and injections can resolve the issue. Surgery may be recommended to treat more severe herniations with nerve compressions.
Deformities of the spine or chest can be associated with other conditions, such as Prader-Willi syndrome, Jeune syndrome, congenital rib fusions, Down syndrome, Marfan syndrome, Ehlers-Danlos syndrome, Rett syndrome, Friedreich’s ataxia, osteogenesis imperfecta and achondroplasia.
Chronic spine injuries are spine injuries that are ongoing. This can be caused by muscle strains and overuse, but constant pain could be a sign of something more serious.
Up to 50% of teens will experience back pain before the age of 20. Most back pain will resolve without treatment. In children age 10 and under, back pain is less uncommon unless there is a specific injury. In fact, the most common cause is constipation. If your child or teen has ongoing pain, consider setting up an appointment to be seen by a doctor.
Common sources of back pain in children and adolescents include:
- Overuse/muscle strains
- Stress fractures (spondylolysis)
- Scheuermann’s kyphosis
- Herniated disc
Childhood back pain can be caused by a variety of issues ranging from normal growing pains to activity-related injuries requiring urgent treatment. Seek out the care of a pediatric orthopedic specialist if your child has any of these symptoms:
- Constant back pain
- Pain that’s only in one specific area
- Pain that requires pain medication
- Pain that limits activities
- Pain associated with fevers, chills and weight loss
In the adolescent age group, back pain is very common and is usually concentrated across the middle of the lower back—and may be noticed especially when sitting or standing for long time periods. You may also notice that your child slouches more often and insists it hurts to sit up straight.
It’s normal for a teen to experience aches right after a growth spurt—muscles typically grow strong before they grow long—but these aches rarely require pain medication or limit activity.
In order to stop the backache, your child may need to build up back and core strength, and a short course of physical therapy may be helpful.
Back pain is an extremely broad topic and may or may not be due to the back itself. Your child’s doctor will complete a physical examination and ask several questions to determine the cause and location of the pain. If necessary, X-rays will be ordered during the initial visit, and then imaging tests and blood work may be recommended at subsequent visits if the cause is still not clear.
How Do Doctors Diagnose Spine Problems?
Our spine specialists treat thousands of growing spines each year, so we understand what to look for in babies, kids and teens.
We work closely with other pediatric specialists to review diagnostic tests that may include:
- A thorough medical history and physical examination
- Routine radiographs with low-dose imaging, such as X-rays
- An MRI
- A low-dose CT scan
- An ultrasound or a bone scan
Our pediatric radiologists receive advanced training, as well as following guidelines and protocols like dose-reducing technology that allows us to cut CT and X-ray radiation exposure by more than 50% compared to adult facilities.
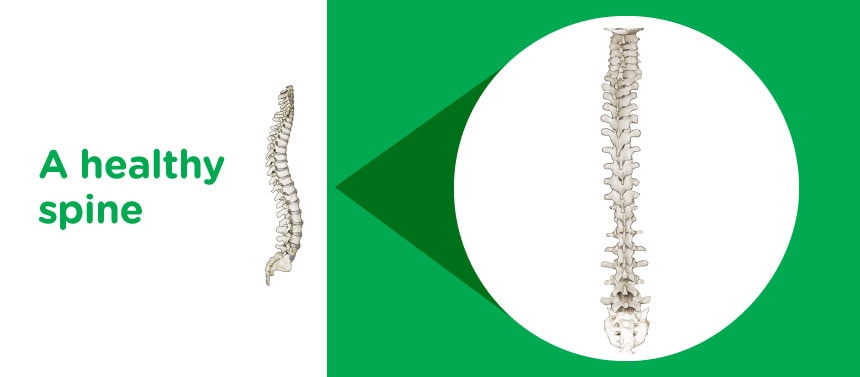
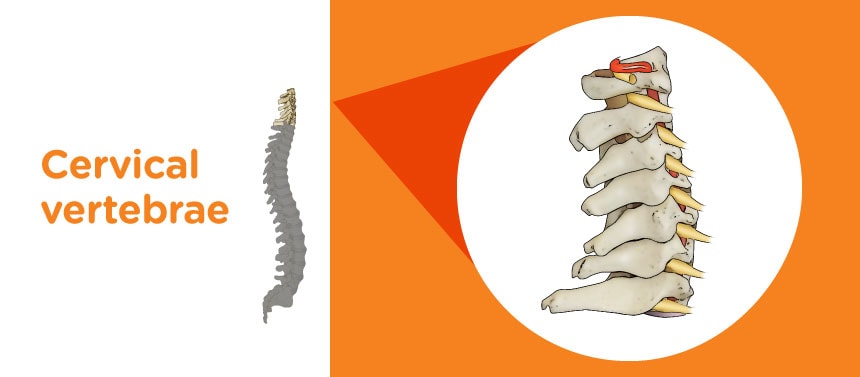
A Closer Look at Your Child's Spine
When our pediatric spine specialists are evaluating your child's spine, we are actually examining several segments of the spine, looking for curves that would help us diagnose your child's spine condition. See the different segments that make up your child's spine, and how the spine can change as your child grows.






What Are Treatments for Spine Problems?
Most kids and teens who come to Children’s for spine care won’t need spine surgery. If your child does need surgery, it’s important to bring your child to a pediatric spine specialist who understands your child’s condition and how it can change as they continue growing. More parents trust Children’s for their child’s spine surgery than anywhere else in Georgia*.
Treatment options for pediatric spine conditions and injuries may include:
- Medication
- Casting or bracing (orthotics)
- Pain management
- Physical therapy and sports physical therapy
- Spinal rest (your child may need to stop some activities while healing)
- Spine surgery
Spine bracing
Spine bracing is used to help prevent curves in the spine from getting larger as your child grows. Generally, curves less than 20 degrees don’t require treatment, since most do not worsen, but children whose curve is larger than 20 degrees are candidates for either part-time bracing (approximately 16 hours a day) or night bracing. Braces do not make curves go away but may prevent the curve in your child’s spine from worsening.
For some children, bracing may not be the best treatment. This may be because of the spine’s curve type, spine stiffness, the spine’s remaining growth, other medical problems or previous surgeries. These are each considered to help our specialists determine which treatment is best for your child’s spine.


Spine Concierge for Spine Patients and Parents
We want our patients and families to have the best possible experience during their spine surgery journey.
Concierge services
Our dedicated concierge team includes a spine program manager who helps coordinate a patient’s experience by providing complete follow-up care and helping make sure families have the information and resources they need before, during and after care. The spine program manager also serves as a single point of contact for your child and their primary care provider.
The spine program manager will help coordinate care by:
- Providing information about lodging and key contacts for those who live outside metro Atlanta.
- Arranging travel accommodations to Atlanta and transportation while in Atlanta.
- Helping families navigate the hospitals and escorting them as needed.
- Assisting with the hospital intake process and clinic visits.
- Writing treatment plans for your child or teen’s referring provider.
- Assisting in arranging the use of durable medical equipment after your child or teen is released from the hospital.
- Coordinating interpretation services.
- Coordinating financial planning with insurance companies.
- Following up with you after your child or teen’s procedure or visit.
- Communicating and coordinating requests for your child or teen’s referring provider.
Contact concierge services at 404-255-1933.
The Scoliosis and Spine Program at Children’s is led by Nicholas D. Fletcher, MD, Medical Director, and Joshua Murphy, MD, Medical Director, Spine Quality and Outcomes.
We know that you want to bring your child to the best pediatric spine specialists. We work closely with specialists from across the country and around the world to help establish best practices for pediatric spine care, and we are on the forefront of advanced technologies. Doctors in our Scoliosis and Spine Program also collaborate with neurosurgeons, anesthesiologists, physiatrists and other specially trained physicians to care for kids, teens and young adults with complex neurological spine disorders, like certain types of scoliosis. Our Orthopedics Program and Neurology and Neurosurgery Program are both nationally ranked, combining experience and specialized training from two of the top programs in the Southeast to treat chronic back and neck pain, herniated discs, spinal cord tumors and degeneration and other conditions in patients from 0 to 18 years old.
Orthopedic surgeons:
- Jed Axelrod, MD
- Robert W. Bruce Jr., MD
- Dennis P. Devito, MD
- Jorge A. Fabregas, MD
- Nicholas D. Fletcher, MD
- Denver B. Kraft, MD
- Joshua Murphy, MD
- Michael L. Schmitz, MD
Orthopedist:
Certified prosthetists-orthotists:
- Karl Barner, CPO, LPO
- C. Leigh Davis, MSPO, CPO, LPO, FAAOP
- Brian Emling, MSPO, CPO, LPO
- Julia Eubanks, MSPO, CPO, LPO
- Jen Galbraith, MSPO, CPO, LPO
- Julie Hantak, MSPO, CPO, LPO
- Rebecca Hernandez, CPO, LPO
- Mark Holowka, MSPO, CPO, LPO, FAAOP
- Greg Kowalski, MSPO, CPO, LPO
- Laura Klagstad, MSPO, CPO, LPO
- Lauren Levinson, MSPO, CPO, LPO
- Elizabeth McCaslin, MSPO, CPO, LPO
- Victoria Moses, MSPO, CPO, LPO
- Rebecca Urquhart, MSPO, CPO, LPO
- Kris Urbanovitch, MSPO, CPO, LPO
- Emma Watson, MSPO, CPO, LPO
- Richard Welling, MSPO, CPO, LPO
Certified orthotists:
- Jessica Corso, CO, LO, FAAOP
- Gillian Munro, MSPO, CO, LO
Certified orthotic assistants:
- Greg Carey, COA
- Megan Shulk, COA










*Pediatric Health Information System (2025), as prepared by the Children’s Hospital Association. This report compares clinical data annually from pediatric hospitals in the U.S.
**No. 9 on the U.S. News & World Report “Best Children’s Hospitals” list for 2025-26.
Contact Us 404-255-1933